Slowly and over the period of many years I saw my dad’s right-hand turn into a permanent and immobile open fist. At first the tissue around his tendons started to harden. When I touched it, they felt strange, like a “living rock”. Then his corresponding little and ring fingers started to pull inwards and became gradually stuck in a permanent and contracted position. He never talked about pain as was his way. Eventually it bothered him to not be able to wash his face anymore. He grew tired of scratching his cheeks with his fingernails every time he tried. He opted for amputation of his fingers. That was that.
Dupuytren’s Contracture (DC) is a connective tissue disorder that affects the palm. The disease primarily affects males from Northern European ancestry. Historical records date the condition back as far as the Vikings.
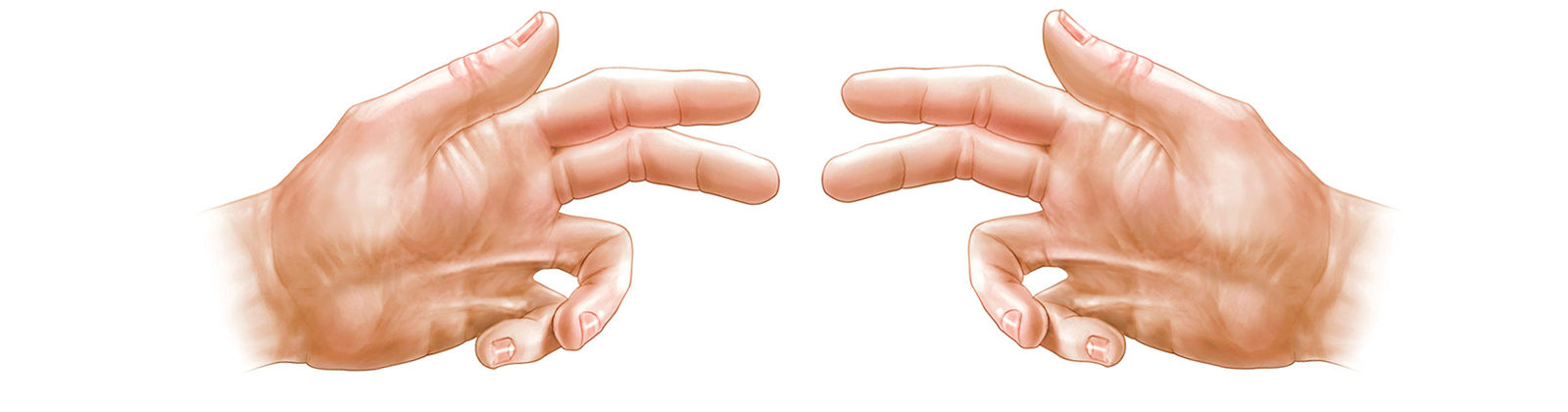
Signs of DC begin very slowly and over a period of years, causing a thick build-up of hard and scar-like tissues surrounding the tendons of the palm. As a result, the fingers (mostly the little and ring fingers) closest to the affected tendons begin to contract, leaving the hand in permanent misconfiguration or claw-like posture. The condition may be painless in some and painful in others, but all DC patients experience disability from the disfigured and immobile fingers.
DC is a chronic degenerative condition whose causes are poorly understood. Modern medicine has no cure and treatment is limited to pharmaceuticals, surgery, or radiation. Drugs such as collagen preparations are injected directly into the affected tissue. Topical surgeries can range from breaking up the scar-like tissue using a needle (aponeurotomy) to complete amputation of the contracted fingers. Also used, especially in their earlier stages, are radiation therapies using ionizing radiation or electron irradiation. Each treatment is costly and can produce mild to serious adverse effects.
Studies suggest that the condition may have two primary underlying causes.1
One, a genetic predisposition called an apoptosis-resistant myofibroblast. Here scientists basically posit that old connective tissue cells that were initially called in to support an injury or inflammation, aren’t self-destructing like they are supposed to after the acute injury is healed. As these cells accumulate, they cause a hardening of the affected tissue.
And two, free radical damage caused by microangiopathy, or small blood vessel disease, that makes it progressively harder for the body to bring life-sustaining support in the form of oxygen (hypoxia) and nutrients to the affected tissues sites in the palm.
Meta-analysis of relevant studies also suggests contributing factors such as alcoholism, diabetes, immune deficiencies, pharmaceutical anticonvulsants, and heavy smoking. It had also been posited that repeated physical actions such as rowing (Viking), using vibrating tools, rock climbing, or hard manual labor may increase disease development in susceptible patients.2
Now a new animal study (2016) conducted by scientists at the University of Cordova, Spain discovers that a CBD-based CB2 activating semi-synthetic cannabinoid (VCE-004.8) was able to mitigate both myofibroblasts and microangiopathy in a similar connective tissue disease of the skin called scleroderma.3
Systemic sclerosis or scleroderma has a very similar underlying pathology and symptomology as Dupuytren’s Contracture, particularly a progressive thickening of the affected tissue and small vessel disease causing hypoxia.
VCE-004.8 treatment (injected into the affected tissue of mice) reduced the accumulated thickness of the skin, blood vessel collagen accumulation, and prevented mast cell degranulation and macrophage infiltration in the skin thus improving movement, build-up, and the delivery of nutrients and oxygen.
To date no controlled human or animal studies have been conducted on DC itself with one exception.
John Lovejoy, D.O. reported on the case of a 46-year-old carpenter with Dupuytren’s Contracture, who developed symptoms over a period of years resulting in the contraction of his right third finger making it more and more difficult to use a hammer.4
Lovejoy reports that the patient self-treated nightly with a homemade topical cream of cannabis (untested, but with an apparent high THC:CBD ratio) covered with a latex glove for the duration of the night. In the morning the patient would wash his hand and go about his day.
Results after a few weeks of topical application were significant and the patient’s contracture had almost completely resolved.
Lovejoy examined the patient one year after treatment began and discovered no residual deformity, contraction, lack of motion, or pain. The patient’s hand was fully functional without any observable deficits.
I just wish I had this information to pass on to my father before he had his two fingers amputated.
1 Nunn AC., Schreuder FB. Dupuytren’s contracture: emerging insight into a Viking disease. Hand Surg. 2014;19(3):481090.
2 Descatha, Alexis et al. Heavy Manual Work, Exposure to Vibration and Dupuytren’s Disease? Results of a Surveillance Program for Musculoskeletal Disorders. Occupational and Environmental Medicine 69.4 (2012): 296–299. PMC. Web. 29 Mar. 2016.
3 Del Río, Carmen et al. The Cannabinoid Quinol VCE-004.8 Alleviates Bleomycin-Induced Scleroderma and Exerts Potent Antifibrotic Effects through Peroxisome Proliferator-Activated Receptor-Γ and CB2 Pathways. Scientific Reports 6 (2016): 21703. PMC. Web. 29 Mar. 2016.
4 John Lovejoy D.O., Dupuytren’s Contracture: Case Study. Published in O’Shaughnessy’s. Winter 2015/16 pg.13
