
Why opioids can kill and why natural cannabinoids do not
By now everybody knows that opioid overdoses can be fatal. What you may not know is that most opioid overdose-related deaths are due to respiratory arrest. That is, once an opioid enters the system in an excessive dosage—via injection, inhalation, snorting, ingestion, or direct application to the skin (think fentanyl patches)—it produces a sedation so intense that the muscles responsible for maintaining respiration simply cease to function, causing inadequate tissue perfusion or shock. If no antidote (i.e., Narcan) is administered, brain death occurs within 5 minutes. Complete physiological death occurs at or around 10 minutes after the last inhalation was taken.
This does not happen with cannabis. There is no respiratory arrest with the use of cannabis, even if taken at very large dosages that may produce a number of adverse effects such as anxiety or a panic attack, for example, or seeming paralysis of many muscles (think “couch-lock effect)—effects that could well be considered those of an overdose. So how is it that opioids can cause respiratory arrest and death and natural cannabinoids do not?
One explanation you will commonly come across is the suggestion that there are no cannabinoid receptors in the oldest part of the brain, the hindbrain, which is responsible for regulating essential functions such as heart rate and respiration. This answer, however, is not the best possible answer. In fact, as a number of peer-reviewed studies have shown, cannabinoid receptors are present in various portions of the hindbrain (including portion of the medulla oblongata).1-6
Research conducted on animals at the University of Hannover, Germany (2017) discovered that cannabinoid receptor sites are located even in the lowest portion of the hindbrain, the medulla oblongata. More specifically, the experiment shows dense CB1 receptor populations surrounding the neuronal bodies of the nucleus of the spinal tract of the trigeminus, which receives input from the 10th cranial nerve.7 The latter is also called the vagus nerve or the pneumogastric nerve in reference to its interface with the parasympathetic control of the heart, digestive functions, and—relevant to this article—the lungs.
You may notice in the headline that we refer to natural cannabinoids. This is an important distinction between naturally occurring compounds and those made by synthetic means. Why is that distinction important? You may know about recent news reports that clearly implicate synthetic cannabinoids in overdoses so severe that they caused organ failure and even death. The reasons why synthetic cannabinoids are more dangerous than natural ones are based in the same physiology by which opioids can kill, and natural cannabinoids cannot. It is the concept of binding efficacy.
This pharmacological concept describes the measurable strength with which a compound such as an opioid, or a cannabinoid such as THC, binds to a particular receptor in the human body (in this case, the opioid receptor mu and the cannabinoid receptor CB1), thereby determining the type and duration of the effect it will produce. The strength or weakness of a compound (the binding efficacy at a receptor, as well as the duration and intensity of the bond, determine the nature of the resulting action (e.g. anti-inflammatory, respiratory depression, changes in cognitive function).
Binding Efficacy is mostly measured by the equilibrium inhibition constant (Ki), and the unit of measurement is so extremely small that it is expressed in nano Molar (nM) units, which represents a factor of one billionth or 0.000 000 001 or 10-9. It is important to understand that the larger the nM number, the weaker the effect and vice versa.
Consider this: Virtually all opioids and a great many synthetic cannabinoids have a strong efficacy for their receptor sites—so strong it is capable of causing death. Meanwhile, naturally occurring cannabinoids (e.g. THC, CBD, anandamide) have a limited range of moderate to very weak binding efficacy at their receptors.
In the following graphic, notice on the left (in red) that all listed opioids have a high efficacy at the mu receptor site. Note on the right that only synthetic cannabinoids have a strong efficacy at the cannabinoid receptor CB1 and as such may present a danger to health and well-being. Those man-made cannabinoids listed are but a few examples of literally thousands of synthetics used in research. However, a number of them have been used in dangerous proportions in products such as “K2”or “Spice,” for example, which are readily available for purchase on the internet and have caused a number of severe medical problems in users and some deaths.
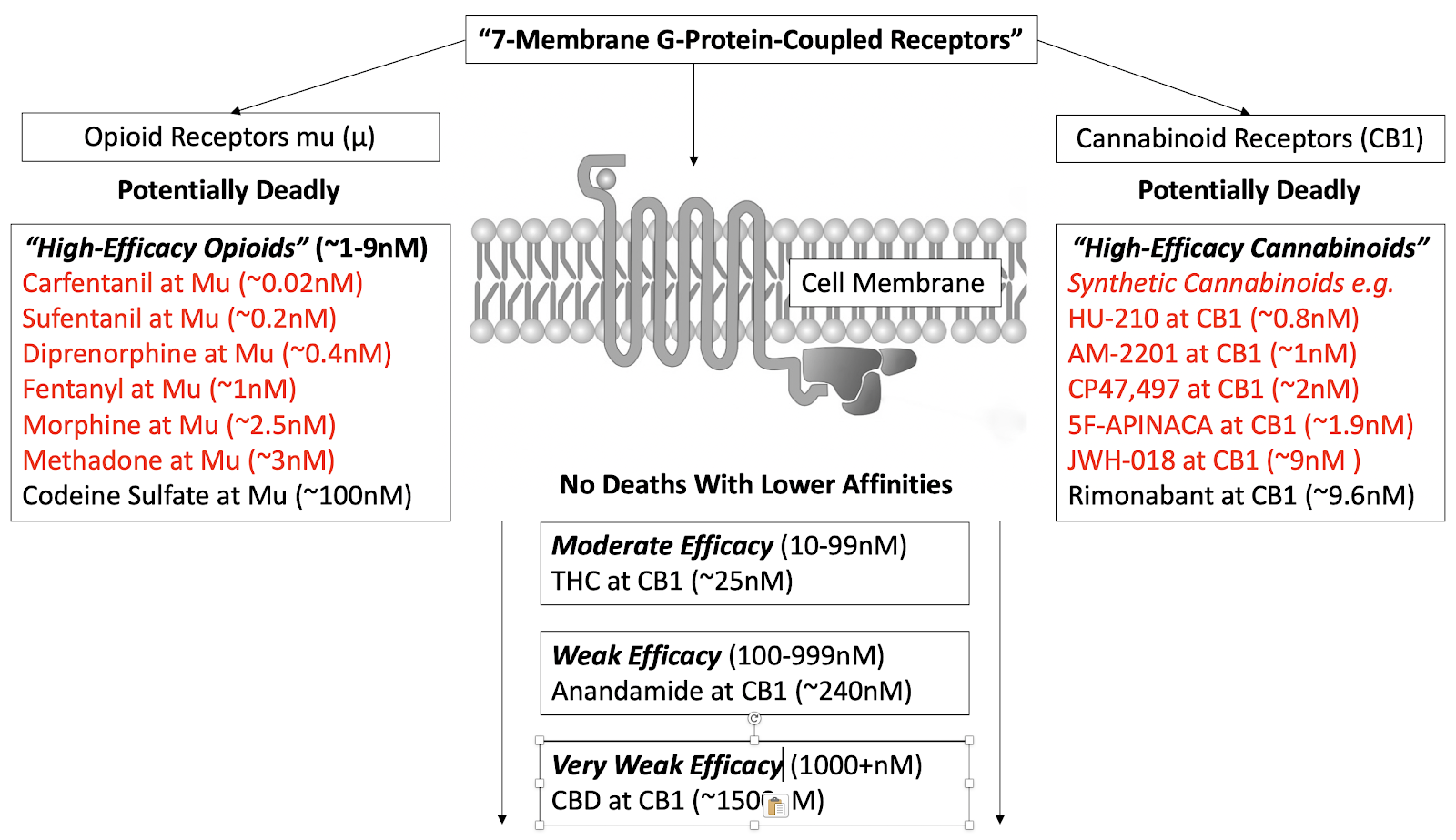
Graphic 1. Efficacies of various opioids and cannabinoids at “7-membrane g-protein-coupled receptor sites”: opioid receptor (mu) and cannabinoid receptor (CB1). The larger the nM number, the weaker the effect and vice versa. Ki values are averages taken from the Psychoactive Drug Screening Program (PDSP). This database is a public domain repository of published Ki efficacy values at various receptor sites. https://pdsp.unc.edu/databases/kidb.php
The reader is remined that the larger the nM number, the weaker the effect and vice versa.
In direct contrast to the hazardous synthetics, naturally occurring cannabinoids like those produced by cannabis (e.g. THC or CBD; see center boxes of graphic), endocannabinoids produced by the human body (e.g. anandamide, 2-AG) and cannabinomimetics of other plants such as liverwort, echinacea, or spices that contain the terpene beta-caryophyllene (which binds with CB2) all have a moderate to very weak efficacy and as such are not life-threatening, even at dosages that might produce adverse effects.
Let me emphasize that just because certain natural cannabinoids are moderate or weak in their binding efficacy to receptors in our body does not mean they are weak in the potential therapeutic effects they can produce. The moderate efficacy of THC at CB1 is strong enough to produce a great number of beneficial healing effects such as alleviating pain, nausea and vomiting, stress, and allergic asthma, for example. However, since the receptor efficacy of THC at CB1 is moderate (~25nM), even with a very high dosage there will be no respiratory arrest or severe organ failure with fatal outcomes like those attributed to high- efficacy opioids or high- efficacy synthetic cannabinoids.
For the curious, here is an estimate of the dosage it would take to produce a deadly response using cannabis. A laboratory study conducted as early as 1973 reported the median lethal dose of oral THC in rats as 800–1900 mg/kg, depending on the sex and genetic strain of the animal.8 If body weight is used as the sole criterion, this study suggests that 200 grams of herb per kilogram of body weight is required to approach a lethal dose in humans. Accordingly, a person weighing 70 kg or 154 lbs. would need to consume 14 kg of herb to approach a fatal dose. In another later study (2004), researchers were much more conservative, stating “628 kg of cannabis would have to be smoked in 15 minutes to induce a lethal effect.”9
So, in summary, this comparison centering on harm reduction makes it clear that moderate to very low-efficacy cannabis or natural cannabis-containing products are safer than high-efficacy opioids. However, since cannabis can cause changes in cognition that can produce adverse effects and lead to unsafe choices with potentially fatal outcomes, it is appropriate to say that naturally occurring cannabis is neither dangerous nor benign.
The more you know about the controllable variables around cannabis and its potential effects on the body and the mind, the more you are able to generate the specific mood-elevating effects or reduction in symptoms you are looking for. These controllable variables center on knowledge about the chemotypes of cannabis, their sub-ratios, the form of cannabis, the dosage of THC and CBD in particular, the presence of other plant constituents and the synergistic effects they are likely to produce, and finally the feedback you gain from your experience with it.
1 Tsou K, Brown S, Sañudo-Peña MC, Mackie K, and Walker JM. Immunohistochemical distribution of cannabinoid CB1 receptors in the rat central nervous system. Neuroscience. 1998 Mar;83(2):393-411.
2 Wang T, Li GQ, Zhang HP, Zhang Y, and Li Q. Overactivation of cannabinoid receptor type 1 in rostral ventrolateral medulla promotes cardiovascular responses in spontaneously hypertensive rats. J Hypertens. 2017 Mar;35(3):538-545.
3 Zou S, Kumar U. Cannabinoid receptors and the endocannabinoid system: Signaling and function in the central nervous system. Int J Mol Sci. 2018;19(3):833. Published 2018 Mar 13.
4 Glass M, Dragunow M, and Faull RL. Cannabinoid receptors in the human brain: A detailed anatomical and quantitative autoradiographic study in the fetal, neonatal and adult human brain. Neuroscience. 1997 Mar;77(2):299-318.
5 Kwok CH, Devonshire IM, Imraish A, et al. Age-dependent plasticity in endocannabinoid modulation of pain processing through postnatal development. Pain. 2017;158(11):2222–2232.
6 Padley JR, Li Q, Pilowsky PM, and Goodchild AK. Cannabinoid receptor activation in the rostral ventrolateral medulla oblongata evokes cardiorespiratory effects in anaesthetized rats. Br J Pharmacol. 2003;140(2):384–394.
7 Freundt-Revilla J, Kegler K, Baumgärtner W, and Tipold A. Spatial distribution of cannabinoid receptor type 1 (CB1) in normal canine central and peripheral nervous system. PLoS One. 2017;12(7):e0181064.
8 Thompson, GR, Rosenkrantz, H, Schaeppi, UH, and Braude, MC. 1973. Comparison of acute oral toxicity of cannabinoids in rats, dogs and monkeys. Toxicol Appl Pharmacol 25:363–72.
9 Carter, Gregory T, Patrick Weydt, Muraco Kyashna-Tocha, and Donald Abrams. 2004 (May). Medicinal Cannabis: Rational guidelines for Dosing. IDrugs 7(5):464–70.
